Navigating prostate cancer, with a pathologist as your guide
SCREENING
Prostate cancer screening usually starts when a man is in his 40s or 50s. It’s done through a blood test that measures for prostate specific antigen, or PSA. That’s an enzyme in the prostate that gets released into the bloodstream.
A man’s PSA level may fluctuate, and a high number does not necessarily mean cancer. A benign enlargement of the prostate, or an infection, can affect the PSA level.
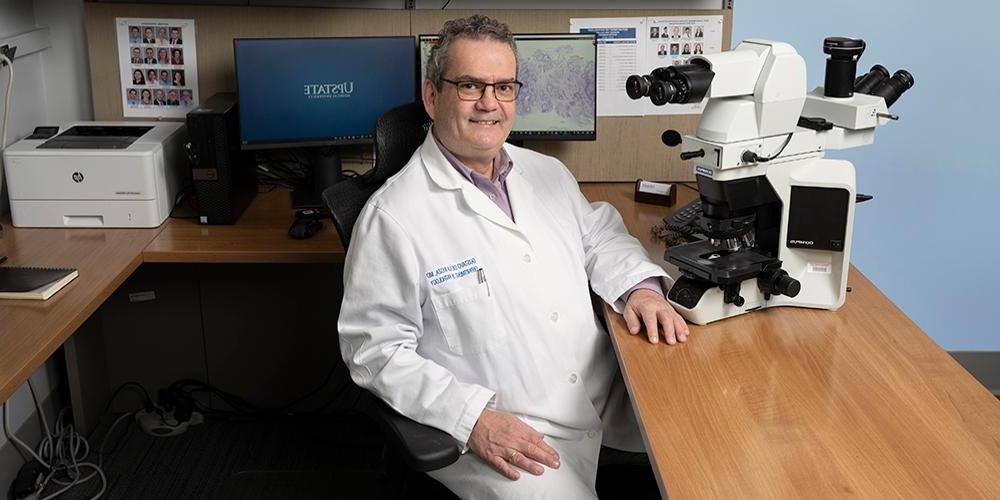
“If we didn’t have prostate specific antigen, we’d be missing a lot of early cancers, and we would only detect those that are already advanced,” says Gustavo de la Roza, MD. He is a professor and vice chair of pathology and the director of anatomic pathology at Upstate.
The prostate, part of the male reproductive system, is located just below the bladder and in front of the rectum. It produces the fluid that makes up part of the semen. Generally, the prostate increases in size as a man ages. About one in eight men will be diagnosed with prostate cancer, which most commonly occurs in men 65 and older.
DIAGNOSIS
Prostate cancer is diagnosed through a biopsy of tissue from the prostate. A pathologist looks at the cells through a microscope. Cancer cells are larger, grow in a haphazard pattern and have certain distinguishing features.
A decade ago, when prostate biopsies included samples from six areas of the prostate, cancers were sometimes missed. De la Roza says modern prostate biopsies include samples from at least a dozen areas, including the periphery of the prostate, where cancer is more likely to be detected, so fewer cancers are missed.
Upstate urologists offer image-guided biopsies, also known as fusion biopsies. It’s a method of targeting a specific lesion in the prostate using ultrasound and magnetic resonance imaging.
(To hear de la Roza go into more detail about prostate cancer in this interview with Upstate’s “The Informed Patient” podcast.)
ANALYSIS
The size of the tumor does not predict a prognosis. The Gleason score and tumor staging do.
The Gleason score — a 1 to 10 grade created in the 1960s by a doctor in Minnesota — remains the most reliable grading system, de la Roza says. It ranks cancers from least aggressive to most aggressive and weighs the risk of the cancer returning after surgery. Basically, the lower the Gleason score, the better.
Clinical staging uses medical images including MRIs and ultrasound.
The Gleason score, the staging, and the PSA levels combine to help urologists determine what treatment options are best for each patient.
TREATMENT
A man who is diagnosed with a prostate cancer that is not aggressive or causing symptoms may opt for active surveillance, an aspect of care that de la Roza says has seen great advancements in recent years.
“It’s not just waiting for something to happen,” he explains. “You are actually actively watching the PSA and deciding when to biopsy again – and that is critical.” He says men in active surveillance receive regular PSA tests and may also undergo imaging and repeat biopsies. “If done this way, the likelihood of missing cancer is much lower.”
POSTOPERATIVE
When prostate cancer is removed through surgery, pathologists like de la Roza examine tissue samples and report whether the cancer was confined to the prostate, spread to surrounding tissues or traveled to distant areas of the body.
This is called TNM staging — T stands for tumor, N for nodes and M for metastases — and it is used worldwide among medical providers who take care of cancer patients.
This article appears in the summer 2023 issue of Cancer Care
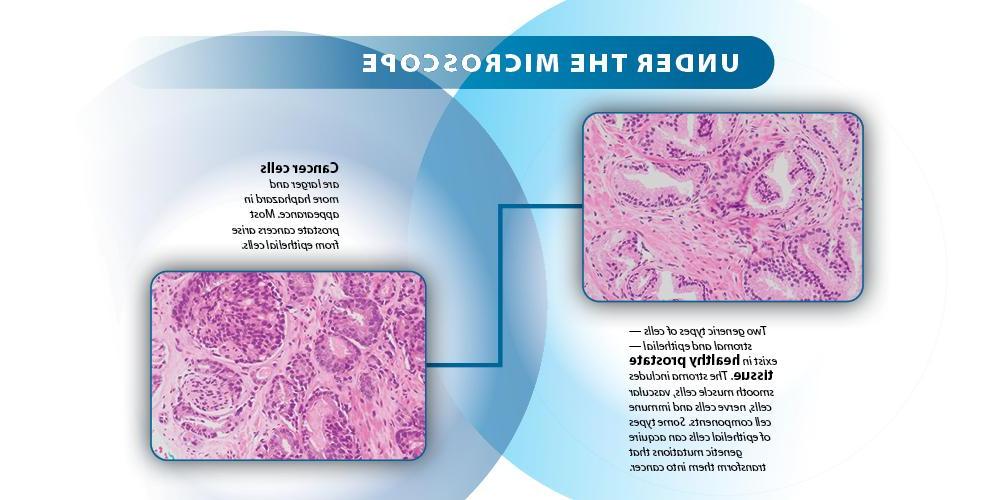 (photos of cancer cells provided by Gustavo de la Roza, MD)
(photos of cancer cells provided by Gustavo de la Roza, MD)